Kidney cancer

Summary/Epidemiology
The kidneys are two organs that filter the blood to remove toxic waste that accumulates in the blood. These wastes are eliminated in the urine that flows from the kidneys into the bladder through the ureters.
Kidney cancer is an uncommon cancer; in Belgium, 1800 new cases are diagnosed annually. Kidney cancer can develop at any age, but is mostly diagnosed between 50 and 70 years of age. The most common type of kidney cancer is adenocarcinoma (90% of all kidney cancers), also called mesonephroma or clear cell carcinoma.
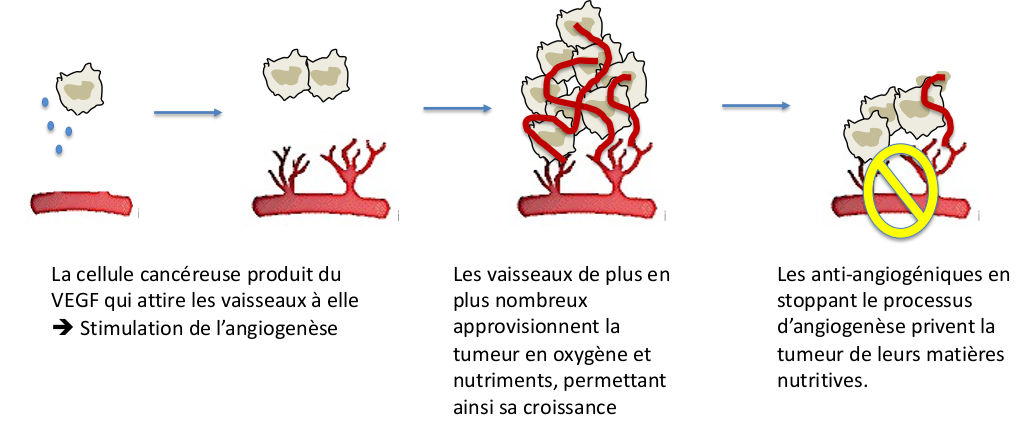
Kidney cancer often develops as a result of an abnormality in a protein, called Von Hippel Lindau, which regulates the formation of vessels (a process called angiogenesis). In 95% of kidney cancers, this Von Hippel Lindau protein is dysfunctional, resulting in excessive and uncontrolled formation of blood vessels that supply oxygen and nutrients to cells that have become cancerous. These blood vessels then participate in the growth of the cancer and the spread of metastases.
Symptoms
Kidney cancer usually grows with few symptoms. It is often diagnosed incidentally, during an abdominal radiological examination (CT scan or ultrasound). As these examinations are very often used by doctors today, more than 50% of cancers are diagnosed at a very localized stage and therefore curable.
As cancers grow, the most common symptoms are blood in the urine, weight loss, and/or abdominal pain.

Treatments
Localized cancer
Small cancers of less than 3 cm can in most cases be monitored by CT scan, MRI, or ultrasound. In case of doubt a biopsy can be performed.
If the tumor is larger but still localized to the kidney, the gold standard treatment is surgery. Whenever possible, the surgeon will remove only the tumor to preserve as much of the kidney tissue as possible. This procedure is called partial nephrectomy. This operation, which used to be quite complex, is now simplified by the use of a DA VINCI surgical robot. Sometimes, if the tumor is too big or invades the excretory cavities, it is necessary to remove the whole kidney, which is called a total nephrectomy.
In some cases, surgery is not an option or the patient is not in good general condition. In these cases, percutaneous ultrasound ablation can be performed by inserting a needle through the skin into the tumor. This treatment is done under radiological guidance.
Advanced cancer
When the cancer is advanced or inoperable, other innovative treatments are proposed:
- Angiogenesis inhibitors are molecules that inhibit the process of angiogenesis, i.e. destroy the vessels that feed the cancer cells. These drugs are administered orally and, although well tolerated, require regular follow-up. Adverse effects, such as fatigue, mouth ulcers, and diarrhea, may occur and are usually easily managed. These anti-angiogenic agents can also have an impact on healthy vessels; it is therefore important to monitor blood pressure, the occurrence of bleeding phenomena, phlebitis, etc. Several molecules are available (Sutent®, Votrient®, Inlyta®, Cabometyx®, Afinitor®, etc.).
- Immunotherapy has revolutionized oncology in general and is commonly used in kidney cancer. Our immune system is basically capable of recognizing and destroying cancer cells through our white blood cells (lymphocytes and macrophages).
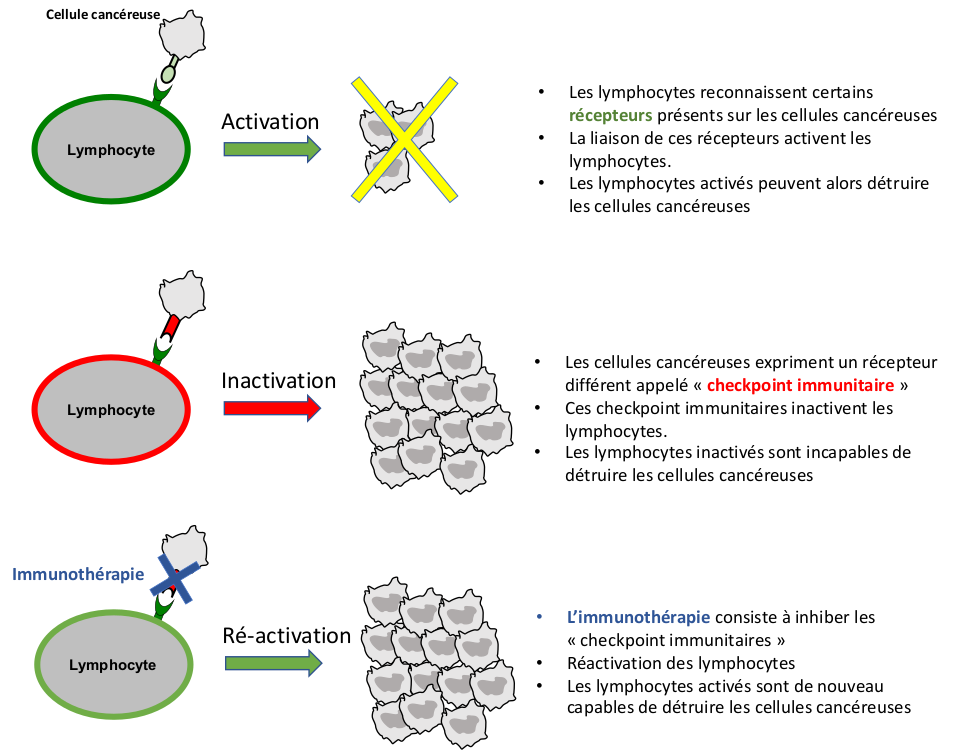
- However, cancer cells can adapt and develop defense mechanisms against our immune system, making themselves invisible to white blood cells (called immune escape). One of the mechanisms developed by cancer cells is to present on their surface a "checkpoint" receptor (a protein that binds to another) called PD-L1, PD-1, or CTLA-4. This protein will bind to white blood cells and inactivate them. The goal of immunotherapy is to re-stimulate the immune system so that it is again able to recognize and destroy cancer cells. These are antibodies that specifically recognize these immune checkpoints and prevent them from inactivating the white blood cells. Numerous molecules are available (Opdivo®, Keytruda®, Tecentriq®) and more are to come. These compounds are administered intravenously every 2 to 3 weeks. Even if they are well tolerated, attention must be paid to autoimmune adverse effects. Indeed, the immune system, excessively stimulated under the effect of immunotherapy, can turn against its host and provoke numerous inflammatory phenomena, either general or directed against a particular organ (diarrhea, skin rash, thyroid or liver function disorders, etc.).
- Recently, we have been using combinations of treatments (anti-angiogenic + immunotherapies), which give a better efficacy but require a regular follow-up because of the adverse effects that can appear. Our coordinating nurses are trained to ensure regular follow-up and to treat these adverse events if they occur; early management makes it easier to deal with them. We obviously follow the recommendations of national and international societies (Figure 4 ESMO 2020 recommendations for the treatment of advanced kidney cancer).
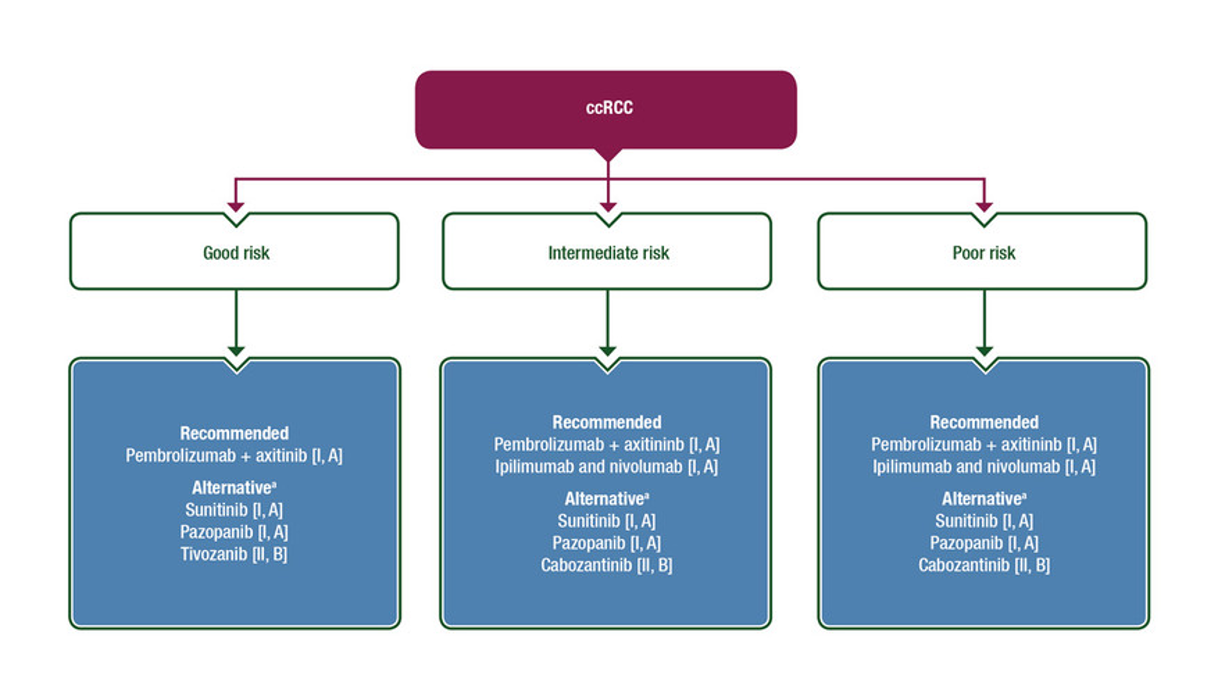
Recommandations de l’ESMO 2020 pour le traitement du cancer du rein avancé
Research and quality of care
Research is important in this still poorly understood cancer. We are participating in multiple international clinical trials evaluating the efficacy of new molecules which, in the future, may become new therapeutic standards. First cases of complete remission of metastases have been described with these therapies, so let's encourage medical research!
We are here to help you through the various steps from screening to treatment. Each specialist (urologist, radiologist, oncologist, radiotherapist) has a specific role in this care. Fortunately, our nurse coordinators provide personalized support for patients from one specialty to the next, being available to answer the smallest of questions and ensuring quality follow-up throughout the treatment, a presence in case of questions and help in case of problems. Psychological help is also systematically offered to support any patient in the difficulties encountered during this journey. In elderly patients, a geriatric evaluation is systematically performed. If this assessment reveals frailties, geriatric interventions and modulation of the cancer treatment are proposed with the collaboration of our geriatric colleagues, in order to ensure an adapted and personalized care of the patient.
Contact
For any further information, or if you would like to make an appointment, please contact the Oncology Care Coordinator at + 32 2 764 35 44.
Doctor

Dr Laurence ANNET

Dr Hélène DANO

Dr Axel FEYAERTS

Pr Jean-Luc GALA

Dr Marco GIZZI

Dr Sofie HEYLEN

Pr François JAMAR

Pr Fréderic E. LECOUVET

Pr Renaud LHOMMEL

Pr Jean-Pascal MACHIELS

Pr Vassiliki PASOGLOU
Dr Barbara SCHMIDT
Pr Emmanuel SERONT

Dr Stéphane THIRY

Pr Bertrand TOMBAL

Dr Julien VAN DAMME

Dr Sandy VAN NIEUWENHOVE

Dr Ad VANDERMEULEN
Paramedical

Karoline AMANN

Naila EL IDRISSI

Kim HENQUIN

Monique KASA VUBU

Christine REMACLE
